

Author's Notes On Chapter 3

In Chapter 1 James, the anaesthetist, insists that Kim finishes Robert’s operation quickly. Bill, the surgical registrar, suggests a quick ex-fix, to which James replies, there is no such thing as a quick ex-fix. Kim agrees to amputate.
Kane suggests at the Monday meeting an ex-fix may have been the better option.
External fixation of fractures has been practiced for thousands of years. In the 5thC BC Hippocrates, described a method illustrated here:

Two rings of leather are firmly attached to the skin either side of the fracture. There are four pouches in each one. Four pieces of green sapling are bent and inserted into the pouches under tension, thus tending to straighten the bone and hold it still. The saplings are stabilised by tying two lengths of twine around them. Imperfect, but much better than nothing.
Over time the methods have improved, and by the end of the 19thC, Hugh Owen Thomas, a Welsh doctor descended from a long line of bonesetters, had perfected splints made of metal, leather and linen that would hold even a fractured femur steady. We were still using these for treatment when I was a young registrar.
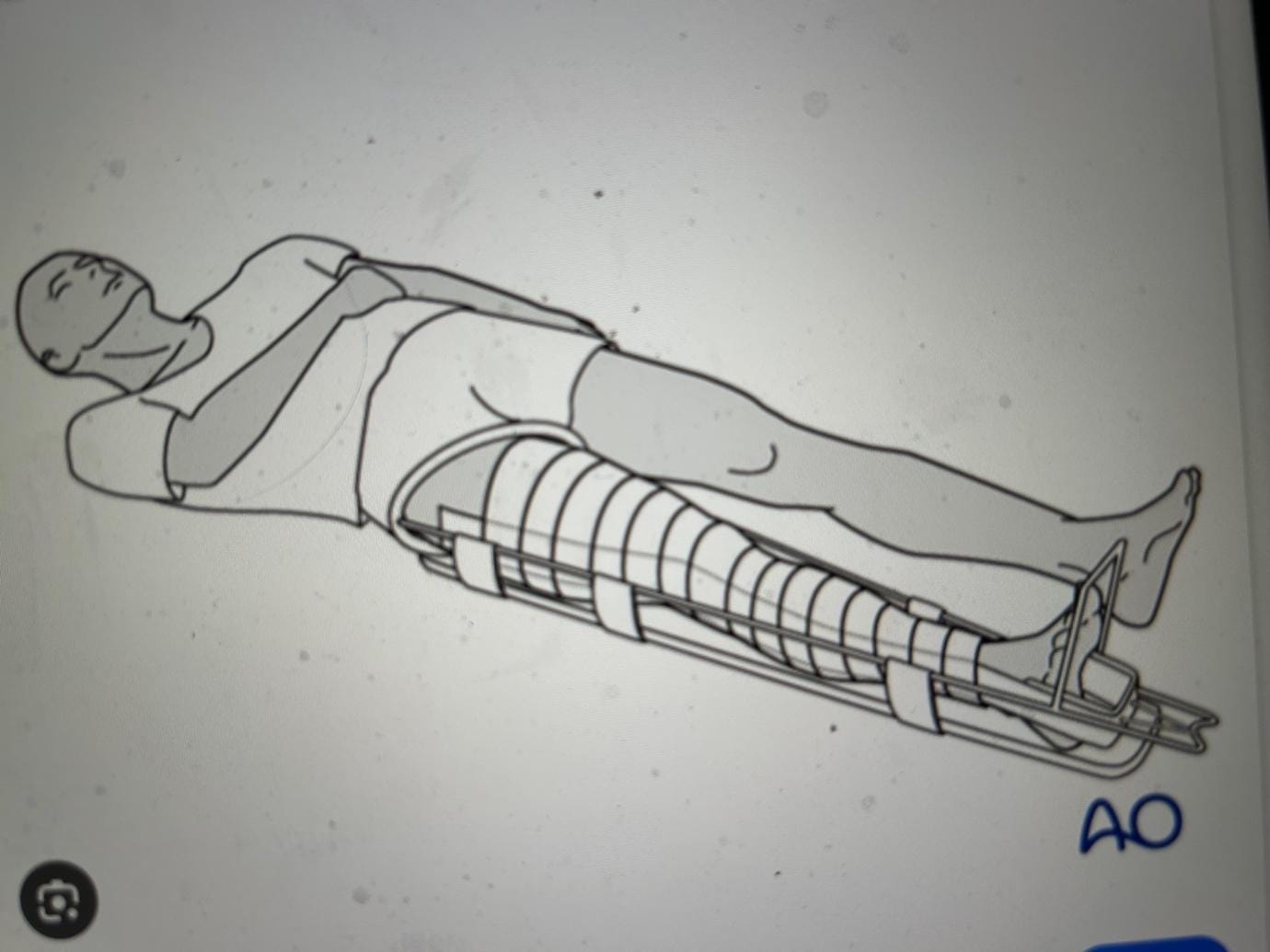
And they continue to be used today for temporary splinting and in children.
We use plaster and it’s modern alternatives as a form of external fixation, but it is very unsatisfactory if there is an open seeping wound underneath that needs constant nursing care or if further surgery is required.
Below is a good method of fixation for a fractured tibia, an internal metal rod, but look at the contamination and small fragments of bone and metal around it. A situation very like Robert’s. This is a better way to manage the fracture than a splint or plaster but there is a big risk of infection around the rod if the wound is wide open.

More flexible methods, using metal pins drilled into the bone and held together by struts, allow the wound to be managed more safely, but it is not very strong. And the pins will eventually loosen, often before the bone has healed.

Kim could have used something like this for Robert and had the option of using more pins and rods for further stability.
Given the circumstances, she accepted the anaesthetists opinion it would have taken too much time, and Robert’s life would be in more peril than it already was.
Robert may have survived with intensive care, his leg eventually healing over many months or years. But if his foot had no feeling, a poor blood supply and limited active movement it would never have functioned as well as a good prosthesis. Eventually, he may have chosen to have an amputation, after two wasted years.
Did she amputate at the right level? Time will tell.
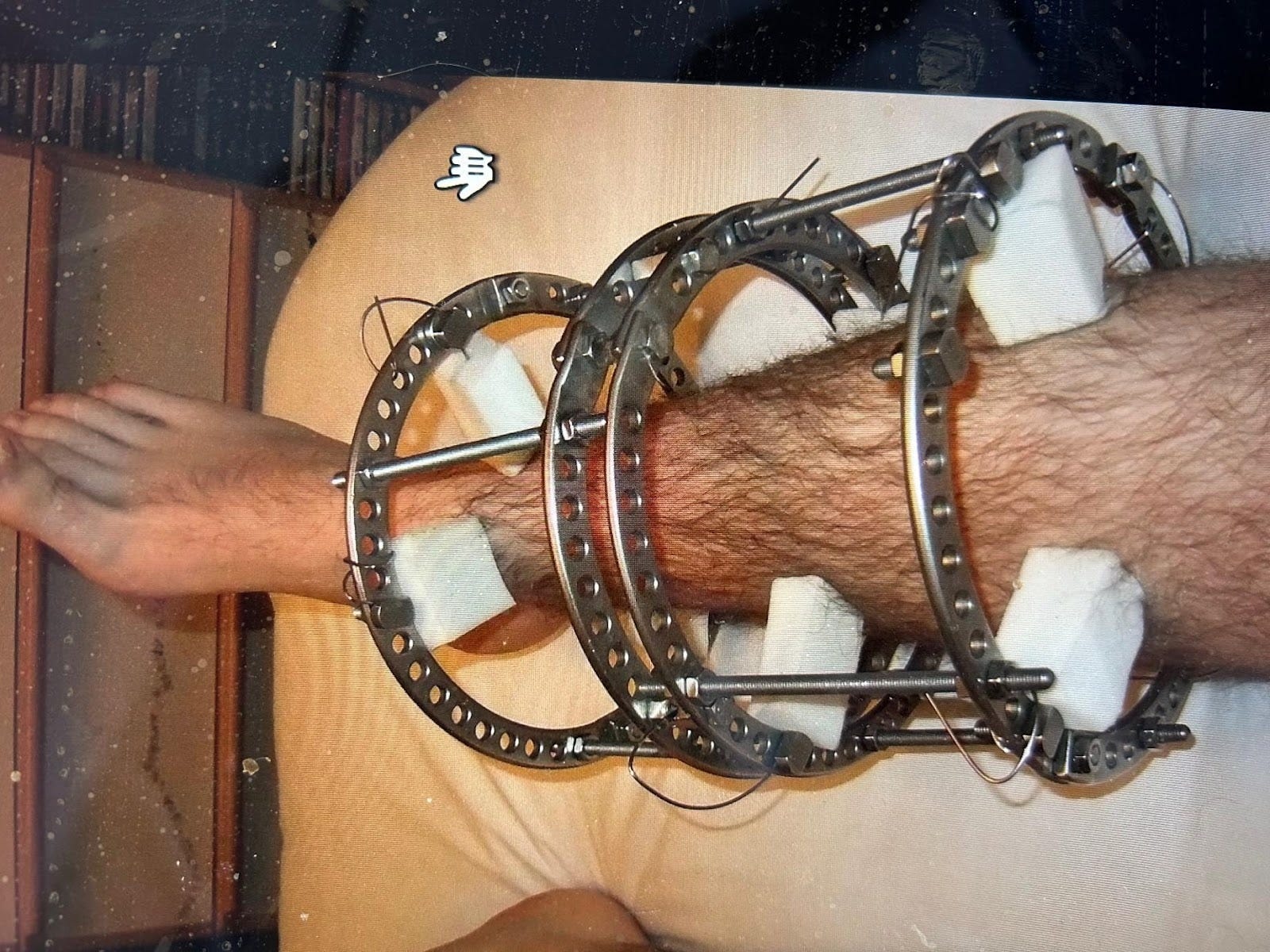
Now we have much more sophisticated ex-fix structures that supply excellent fixation and allow wound care, including subsequent muscle and skin grafting.
Wires and pins extend from the side of circular frames and pass through the bone, above and below the fracture, to the other side of the frame under tension. This gives firm control of the major bone fragments. The frames are firmly attached to each other with struts that can be adjusted to control the fracture length and alignment. You can continue to work on the soft tissues without disturbing the fracture.
However, they take time and skill to apply well.
thank you